| Contributed by Vanessa Tseng, MD, Elijah W. Stommel, MD, PhD, Dept of Neurology and Brent T. Harris, MD, PhD Dept of Pathology (Neuropathology) Dartmouth Medical School and Jayashri Srinivasan MBBS, PhD, Lahey Clinic |
|||
|
|||
CLINICAL HISTORY:
ID: Brothers who developed slowly progressive hypesthesias of the lower extremities, distal weakness and gait ataxia.
HPI:
Two elderly brothers aged 70 and 77 developed insidious onset of paresthesias
and hypesthesias of the lower extremities. Over the course of more than two
years, they also developed mild weakness of the distal lower extremities. However,
the mild lower extremity weakness was overshadowed by the development of significant
imbalance and ataxia. There was no history of toxic heavy metal exposure, auto-immune
disorders, precipitating infections. There was no family history of a polyneuropathy
or any other neurological disorder.
PHYSICAL EXAMINATION:
Mild weakness in bilateral distal lower extremities - 4/5 on MRC grading scale.
5/5 proximal strength
Sensory exam – significant symmetric vibratory and proprioceptive loss
in UE and LE up to knees and wrists, loss of pinprick and temperature less pronounced
DTR – absent throughout
Gait – wide based and severely ataxic.
Romberg sign – present
LAB EXAMINATIONS:
BUN/CR, LFT’s, B12, folate, TSH, RPR – within normal limits
Heavy metal screen – negative
CSF results: high protein, no WBC’s – Brother 1: pro 92, O WBC;
Brother 2: pro 61, O WBC
SPEP: IgM monoclonal gammopathy with kappa light chains
Anti-MAG Ab - positive
GENETIC TESTING:
PMP22 gene, Myelin Protein Zero gene, Connexin 32 gene – without duplication,
sequence change, or point mutations, thereby ruling out hereditary motor sensory
neuropathies (type 1a, 1b and X-linked respectively)
NEUROPHYSIOLOGY FINDINGS:
EMG showed severe demyelinating polyneuropathy with chronic secondary axonal
changes.
Nerve conductions studies showed a disproportional increase in distal latencies.
One of the brothers is taken to surgery where a sural nerve biopsy is performed.
MICROSCOPIC DESCRIPTION:
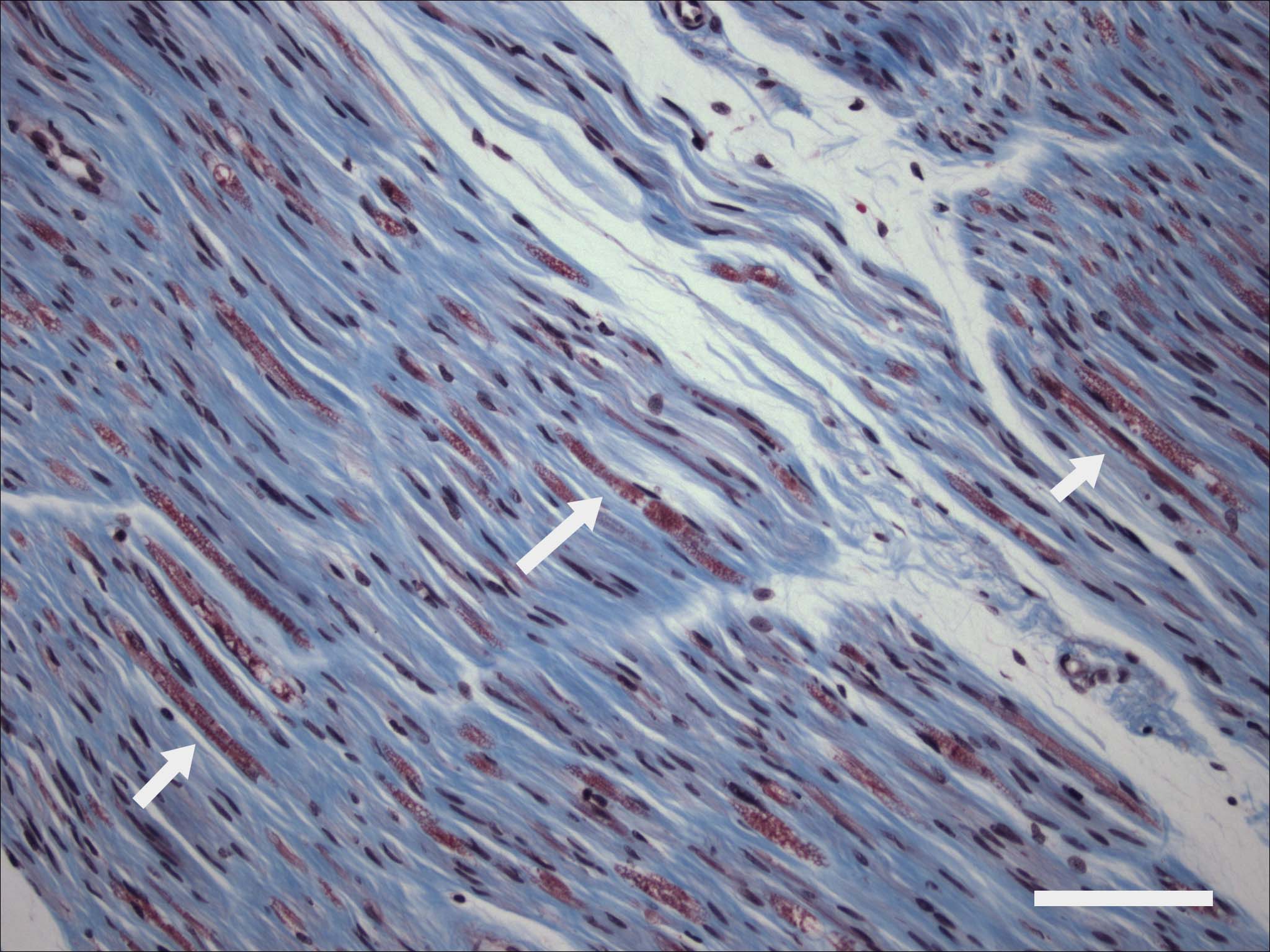
 CLICK ON IMAGES TO ENLARGE
CLICK ON IMAGES TO ENLARGE
(A) Trichrome stain highlights fibrosis and moderate loss of myelinated fibers.
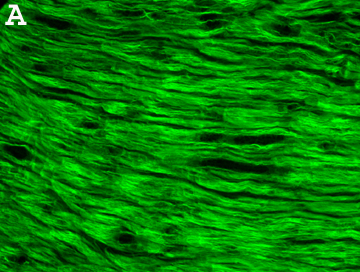
(B) Immunofluorescence staining specific for human IgG displays diffuse, non-specific
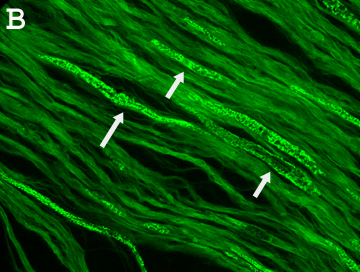
pattern. (C) IgM-specific immunofluorescence staining displays focal, linear
pattern, which probably represents staining of the few remaining myelinated
axons of this sural nerve biopsy.