| Contributed by Brent T. Harris MD, PhD | |
| Department of Pathology (Neuropathology), Dartmouth Medical School |
CLINICAL HISTORY AND RADIOLOGY:


This 50-year-old female is referred for further evaluation of new-onset left facial weakness and an abnormal MRI scan.
She relates a history of 1-2 weeks ago becoming aware of slurring of her speech. She has had related trouble eating and swallowing and is aware of weakness which has persisted to present. On questioning, she and her husband note that she has had headaches over the past 1-1/2 months which she does not typically experience. She denies any abnormal movement or seizure activity. She has not had involvement of her arm or leg, although she does describe having had some aching of her right upper extremity and neck. She has no history of seizures, infection, head trauma, recent foreign travel or other neurologic symptoms. She has been in good health, and her review of systems is otherwise noncontributory apart from having noted some fatigue over the past month. She does not smoke. Her alcohol use is described as "very little." Her family history is unremarkable apart from her mother dying with amyotrophic lateral sclerosis 1-1/2 years ago.
On examination, she is alert, attentive, appropriate, cooperative, and in no obvious discomfort. Her speech is fluent and mildly dysarthric; there are no naming errors. Her pupils are 2 mm, equal, and reactive; funduscopy demonstrates sharp disk margins; venous pulsations are not visualized; visual fields are full to confrontation; extraocular movements are full. Trigeminal sensation is intact to light touch. She has a central left facial paresis. There is no pronator drift. Strength of her upper and lower extremities is full. Tone is full. Sensation of her extremities is intact to light touch. Cerebellar examination shows good finger-to-nose testing bilaterally. Deep tendon reflexes are difficult to elicit throughout. Gait, tandem gait, and station are all within normal limits.
A review of her MRI demonstrates a right frontal lesion with an incompletely enhancing rim. It measures about 3 cm. in diameter, and appears to have a cystic or necrotic center which is diminished in intensity on T1 and bright on T2. There is little surrounding edema associated with this.
Impression: This 50-year-old white female presents with a 1- to 2-week history of left facial weakness associated with a right frontal mass. The differential diagnosis is broad with concern that this represents a tumor. The signal characteristics include the possibility of a cystic component. An infectious process cannot be excluded.
The patient is taken for a stereotactic biopsy of the lesion.
MICROSCOPIC DESCRIPTION:
 CLICK ON IMAGES TO ENLARGE
CLICK ON IMAGES TO ENLARGE
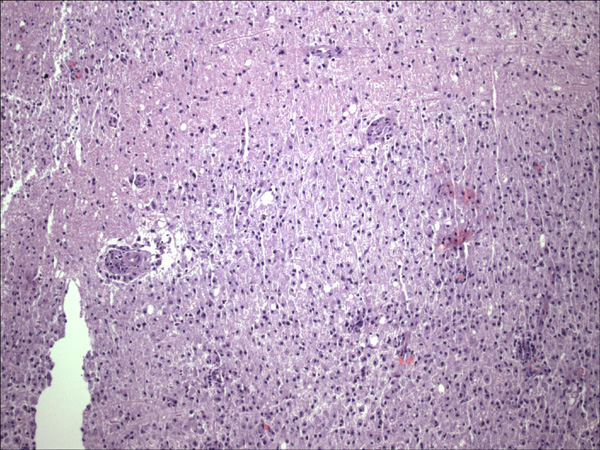
Sections display neural tissue extensively infiltrated with inflammatory cells
composed primarily of lymphocytes and macrophages. There is no acute neutrophil
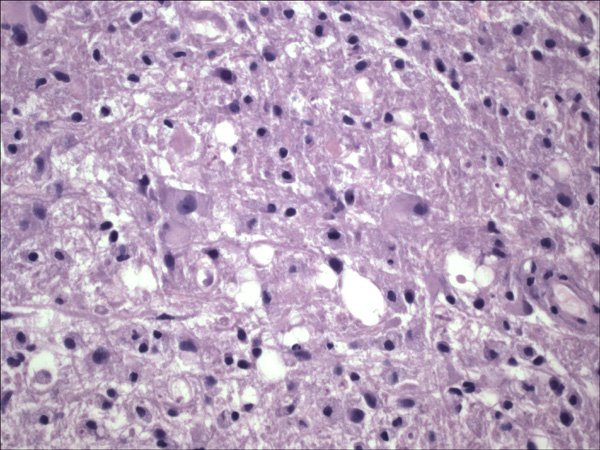
infiltrate. Within some fields, the background neuropil has a loose, ragged
appearance and abundant macrophages with foamy cytoplasm are present. Many of
the vessels have surrounding lymphocytes and macrophages. Special stains for
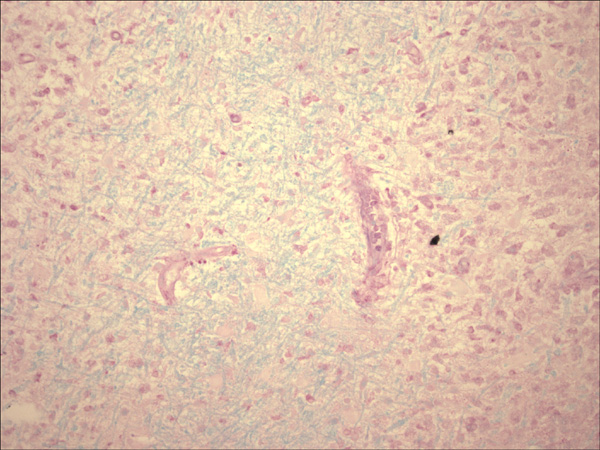
microorganisms (Gram and GMS) do not highlight any organisms. A LFB-PAS
stain highlights some PAS positive material (pink) within perivascular macrophages
. In addition, this stain shows large areas with loss or fragmentation of myelin
(light blue). Immunohistochemical stains for GFAP show an extensive network
of evenly spaced reactive astrocytes within the tissue. Proliferation marker
KI-67 highlights only proliferating inflammatory cells.
{kind=link}
{kind=link}
{kind=link}